Neurodiversity has become a familiar term in psychology, counselling and psychotherapy. The concept was first coined by Kassiane Asasumasu in the early 2000s, and has since gained prominence both in clinical research and as a rallying point for social advocacy. Yet in some clinical spaces, it can be framed too narrowly. It is often reduced to medical diagnoses, and sometimes even symptom lists and behavioural traits, or treated as a clinical category rather than recognised for its wider social, political, and ethical implications.
This limited view completely misses the point.
To understand neurodiversity well, psychologists and other clinicians need to move beyond neurodiversity lite and purely medicalised terminology. Neurodiversity lite refers to a superficial understanding or application of neurodiversity principles. One that emphasises inclusive language and symbolic gestures yet fails to address deeper systemic barriers or advocate for meaningful, structural change. Neurodiversity is not a medical term. It is rooted in the history of marginalised communities and shaped by resistance to narrow ideas of normality.
Clinical knowledge matters when we are specifically talking about neurodevelopmental conditions, which many confuse with neurodiversity. Assessment, formulation and evidence-based support might be relevant for those that are seeking diagnoses, and support.
But neurodiversity is not purely a diagnostic matter. And those of us that work within neurodivergent people, and are, in my case, neurodivergent themselves, when we talk about neurodiversity, we need to be aware of its social injustice roots.
The neurodiversity paradigm is a social movement. It asks us to think about power, exclusion, access, identity and justice. It asks us to notice who gets supported, who gets pathologised and who gets left behind.
This matters because therapy never happens in a vacuum.
People bring their own unique nervous systems, histories, identities and lived realities into the room. They also bring the effects of schools, workplaces, healthcare systems, poverty, racism, sexism, ableism and other forms of structural inequality. If we discuss neurodiversity without discussing these wider forces, we risk offering language without change. We risk paying lip service to inclusion while leaving harmful systems intact. For me, this is one of the clearest signs of neurodiversity lite: using affirming language without pushing for change in the structures that cause harm.
It isn’t easy, particularly for those that are operating within the systems, and the constraints that we have. For example, how do we tackle the support needs of a neurodivergent person in the 6 funded counselling sessions that we might be given on the NHS?
We can still be that voice for change, and call these failings out. And even point clinicians towards processes that do consider wider contexts.
For example, the Power, Meaning, Threat Framework within psychology offers a framework for working with an individual, and those contexts that might have shaped them in a non-pathologising way. It is worth exploring for those in clinical practise, and seeing if the principles are something that will support you, or your clients.
In this particular post, we will look at why neurodiversity must be understood beyond those medical terms, why it should be recognised as a social movement, and what this might mean for psychologists, therapists and counsellors day-to-day.
Moving past neurodiversity site: What neurodiversity means beyond diagnosis
At its simplest, neurodiversity refers to the natural variation in human minds and nervous systems. It challenges the idea that there is one correct or superior way for a brain to work: the neuronormative way. Instead, it sees differences in thinking, processing, communicating, focusing, feeling and relating as part of human diversity.
That sounds straightforward, but the term is often misunderstood. In practice, some people use neurodiversity as shorthand for autism and ADHD alone. Those are important parts of the conversation, but they are far from the whole of it. Neurodiversity is broader than a short list of diagnoses. It invites us to think more widely about how people experience the world and how systems respond to that difference.
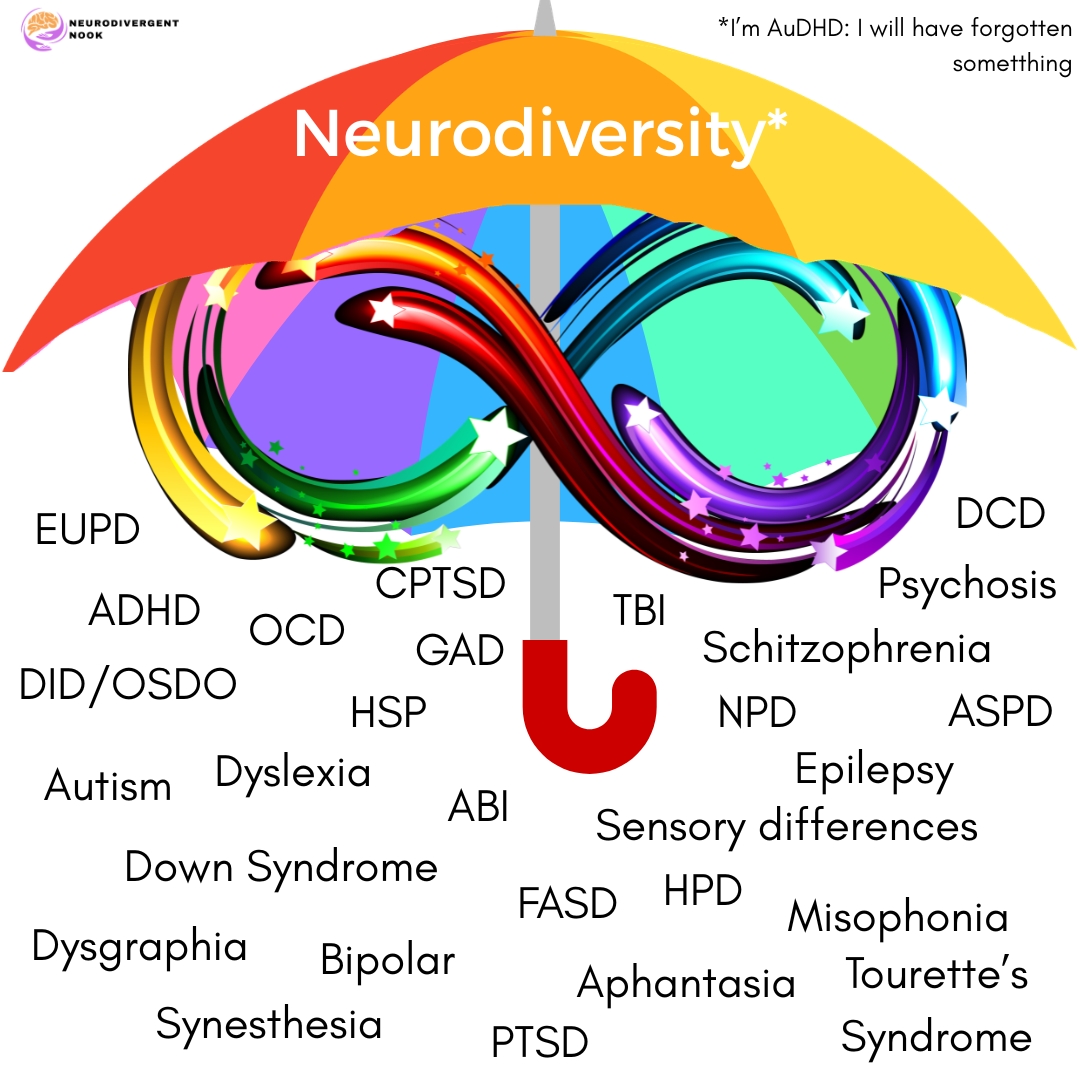
There are many “conditions” that fall under the neurodiversity umbrella as it was intended when it was first proposed. Anything that deviates from the neuronormative standards are considered covered by the term:
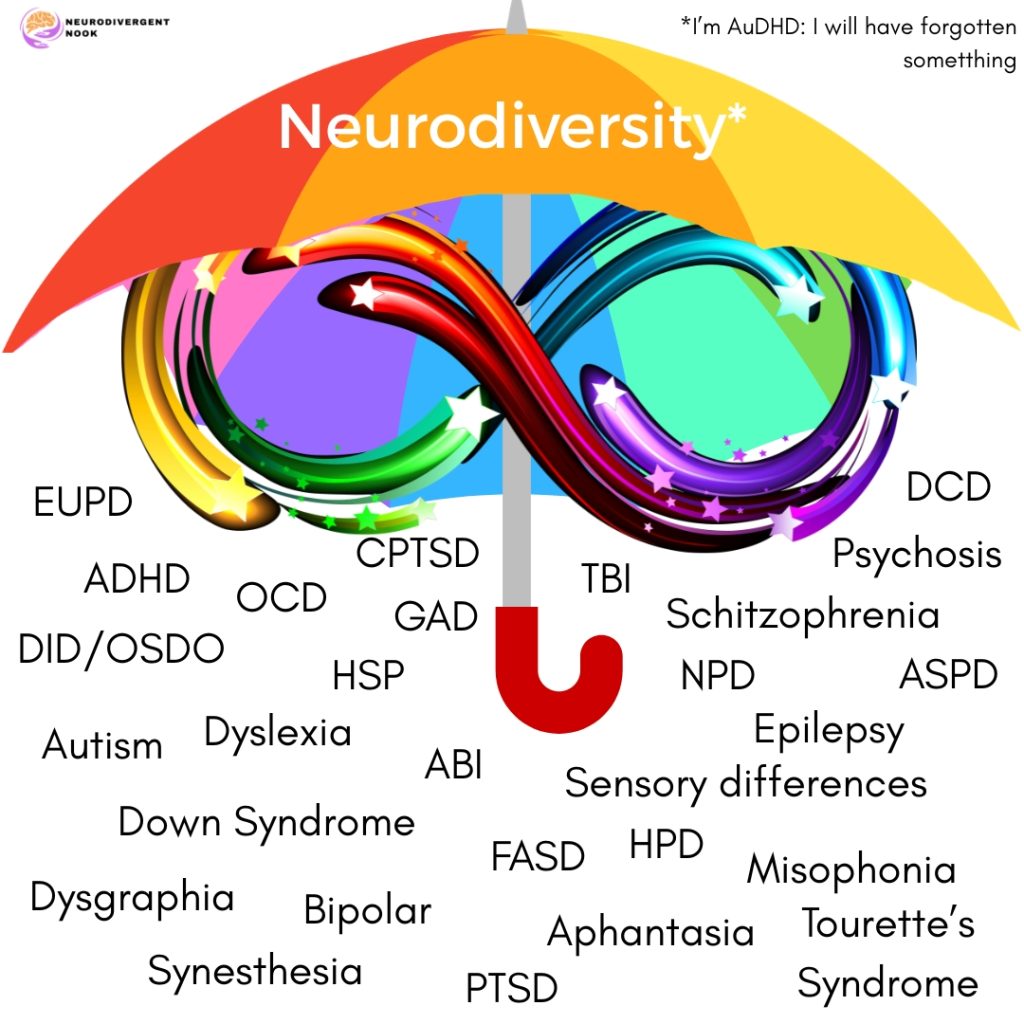
The medical use of the word can tend to focus on deficits, impairments and deviation from a norm, the neuronormative norm that is very specific to psychiatry. And it is always worth remembering that this is a social construct.
For example, many cultures, and thanks to the Hearing Voices Network, don’t necessarily consider hallucinations something to be afraid of, or indeed, something to be “fixed”.
It can be useful for access to legal protection and support to pursue diagnosis. Some find it validating and life-changing. The problem is not medical knowledge itself. The problem comes when medical language becomes the only language we use. Or we feel we are being “done to” and not “with.” The medicalisation of natural human diversity means that we are given the label, and then there are many who try to fix what are seen as difficulties, and deficets, rather than deviations from the norm, which are still inherently value to the human race, and indeed humanity.
When that happens, the person can disappear behind the case formulation and the medicalisation of their identity.
Distress gets interpreted only as dysfunction. Adaptation gets mistaken for pathology. Social barriers get ignored. A client may not be struggling because their brain is different from the neuronormative. They are more likely to be struggling because they are trying to survive in environments that were not built with them in mind.
We are not looking at how their behaviour is giving us clues to an unmet need.
Why neurodiversity is also a social movement
Neurodiversity is not just a descriptive term. It is also tied to activism, advocacy and disability justice. It emerged in response to narrow ideas of normality and to systems that have often excluded, silenced or harmed neurodivergent people.
As a social movement, neurodiversity asks bigger questions than diagnostic manuals can answer. Who defines what counts as normal functioning? Is there indeed a normal? Whose behaviour gets tolerated and whose gets punished? Which people are offered support early, and which are dismissed, misread or criminalised? Who can afford private assessment? Who might be seen as “high functioning” and therefore denied help? Who is labelled “complex” and pushed out of services because that word means they have already been written off as too difficult for the system to support? For a wonderful book about this, do check out Diagnosis Human (affiliate link) by Elle Chappell who writes so eloquently about her daughter, Ella.
These are not abstract questions. They shape real lives. Research and practice have repeatedly shown that many neurodivergent people face delayed diagnosis, poor mental health outcomes, school exclusion, workplace discrimination and barriers to care. These burdens do not fall evenly. Marginalised communities often face compounded disadvantage. Intersectionality pays a huge part in the outcomes for neurodivergent people.
I am a cis white women and know the privilege I have been afforded that has helped me to be able to navigate my neurodivergence without support for half my life. I have had resources, such as money and support, that others simply don’t have access to.
That is what has meant I am where I am today, and it is heart-breaking to see that there are so many that fall through the cracks before we cannot offer the support and resources that they need.
In addition to my own personal story, there are examples of where race, class, gender, sexuality, language and immigration status can all affect whether someone is believed, assessed, understood or supported. Girls and women may be overlooked because of gendered stereotypes. Black children may be punished for traits that might be recognised very differently in white peers. People with fewer financial resources may wait years for assessment or go without it entirely. LGBTQ+ neurodivergent people may face layered misunderstanding in both mental health and community settings.
A justice-based approach to neurodiversity therefore matters. Without it, clinicians may use affirming words while still working inside exclusionary assumptions.
Inclusion does not stop at sensory tools in a waiting room. Fidget toys may indeed help some people. Flexible lighting may help other people. But neurodiversity asks for more than simple cosmetic adjustments. It is asking for structural change.
The limits of a purely medicalised approach
Medicalised language can help name a pattern and open doors to support. But when it dominates practice, several problems can follow.
It centres deficit over context.
A purely medical lens can frame the person as the problem. Difficulties with concentration, social communication, emotional regulation or sensory processing may be seen only as internal faults. The wider environment, and the systems, then escape scrutiny.
We blame the person. We don’t dig deeper.
Context matters.
A client who appears “non-compliant” may be overwhelmed by inaccessible systems. A child described as “oppositional” may be distressed by sensory overload or chronic misunderstanding. An adult who seems “disorganised” may be exhausted from masking, poverty, caring responsibilities or repeated institutional failure. The classic mis representation in autism of lacking empathy, may be someone who is overwhelmed, or struggling to find the words due to Alexythymia.
It can flatten lived experience
Neurodivergent people are not all alike. Diagnosis does not tell us everything about identity, coping, strengths, culture or need. Clinical labels can become blunt instruments when they are used without curiosity or humility. Bias around clinical labels prevents true support if we fail to see the whole person, and just pigeon-whole someone into a diagnostic category.
Psychologists need rich, person-centred understanding. That means listening to lived experience, not just fitting clients into these pre-set categories. It means asking how a person understands themselves, not just how they appear against neuronormative standards.
It may reinforce harmful norms
Many traditional clinical approaches have been shaped by the goal of helping people appear more normal. That can place heavy pressure on clients to mask distress, suppress natural ways of communicating or perform socially acceptable behaviour at great personal cost.
The support we give to neurodivergent people is not to make they more neurotypical: it is to help them understand themselves, and to give them, and those around them, the tools to advocate.
Support should not be judged only by how well someone blends in. A person is not thriving simply because they are easier for others to manage. Quite the contrary. If someone in my therapy room is now asking for adjustments after working with me, that’s a win. Both in terms of their own understanding, and having the confidence to ask for support around challenges, and work with their strengths.
Neurodiversity is more than ADHD and autism
Autism and ADHD are central to many public discussions about neurodiversity, but the conversation cannot end there. If mental health professionals only engage when they hear familiar diagnostic labels, they miss both the breadth of neurodivergent experience and the wider relevance of the framework.
Neurodiversity also matters in relation to learning differences, sensory differences, communication styles, executive functioning, trauma responses, emotional regulation and the complex overlap between mental health and neurodevelopmental conditions. These areas do not fit into tidy boxes. They are often interwoven.

Mental health support is a key part of this picture. Neurodivergent people may experience anxiety, depression, burnout, shame, loneliness and trauma not simply because of intrinsic traits, but because of repeated invalidation, exclusion and unmet needs. If therapists miss that, they may treat the emotional wound while ignoring the conditions that keep reopening it.
This is why understanding neurodiversity requires more than awareness of diagnostic criteria. It requires attention to the social causes of distress, the barriers within services and the gap between what clients need and what systems provide.
What this means for clinicians, therapists and counsellors
Neurodiversity should shape both mindset and method. It is not an optional add-on. It should influence how we formulate problems, build relationships, assess risk, adapt interventions and think about ethics.
Listen for systemic harm
When clients talk about anxiety, low mood or self-doubt, listen for the role of repeated misunderstanding, exclusion or pressure to mask. Distress may be linked to systems that have failed them, and it is vital that we give space to the emotions that this systemic injustice brings up for clients.
Let us consider “What has happened?” and “What contexts is this person trying to survive?” “What meaning have they made from the power they have in their life?”
Avoid superficial inclusion
It is easy to signal awareness without changing practice. A few social media posts, a one-off training session or a neurodiversity-friendly badge on a website do not mean much on their own. Real engagement requires deeper work. If we are serious about moving beyond neurodiversity lite, we have to change practice where we can, not just presentation. We know there are systemic barriers even to this, including budgets, yet we need to start somewhere.
That may include adapting communication, reviewing intake processes, allowing alternative forms of expression, reducing sensory demands, being flexible with eye contact and session structure, and questioning assumptions about emotional expression, rapport, motivation and resistance.
Respect identity and autonomy
Not every client will use the same language for themselves. Some prefer identity-first language, others prefer person-first language. Some value diagnosis, others do not. Some see neurodivergence as central to who they are. Others are still working that out.
Respect means not imposing a single narrative. It also means recognising that self-knowledge matters.
Think intersectionally
Neurodiversity does not exist apart from race, gender, class, disability, sexuality or culture. These identities shape how people are seen and treated. A therapist who ignores that may miss the client’s actual reality.
Intersectional practice helps us understand why some people are diagnosed early and supported well, while others are misunderstood, or never recognised at all.

From awareness to systemic change
If neurodiversity is a social movement, then psychology, therapists and beyond cannot respond only at the level of the individual. We, as mental health professionals, also need to think systemically.
That means advocating for accessible services, fairer assessment pathways and environments that reduce harm rather than create it. It means challenging service designs that reward conformity and penalise difference. It means questioning whose needs are centred in policy, training and clinical norms.
Professional bodies, training courses and services all have a role here. Neurodiversity should not be confined to a small specialist module. It should be integrated into core thinking about development, mental health, ethics, culture and power.
For individual practitioners, systemic change may begin with small but meaningful steps:
- Review whether your practice environment is actually accessible,
- Examine deficit-based language in notes, reports and formulations,
- Seek neurodivergent-led training and writing,
- Build knowledge of how oppression shapes mental health outcomes,
- Adapt therapy so clients do not have to spend energy performing normality, and
- Advocate within teams and organisations for better policies and pathways.
These are not extras. They are part of competent, ethical care that is actively trying to move beyond neurodiversity lite.
A better standard for mental health practice
Psychologists, therapists and counsellors are in a powerful position. We can help shape how distress is understood. We influence whether people feel seen or reduced. We can either reinforce narrow norms or help create more just and humane forms of support.
Understanding neurodiversity beyond medical terms does not mean abandoning clinical rigour. It means broadening it. It means holding diagnosis and social context together. It means recognising that difference is not the same as defect, and every individual has a value to our humanity. It means seeing that many struggles arise not only from internal challenges, but from inaccessible and unequal worlds.
Most of all, it means taking neurodiversity seriously enough to let it change our practice. Not just our vocabulary. Not just our branding. Our practice, and our own way of showing up for neurodivergent people.
If we want to support neurodivergent clients well, we must move beyond the surface. We must listen to lived experience, attend to injustice and work for systemic change. Anything less risks turning a vital social movement into a clinical buzzword.
That is not good enough for our clients. And it should not be good enough for our professions either.
Leave a Reply